Here’s the claim, more or less, that gets repeated across every “here’s where to go now” article since Peptide Sciences reportedly went dark: don’t worry, there are supervised alternatives. Compounded. Dispensed by a licensed pharmacy. 503A. Telehealth platform. Independent licensed providers.
I went looking for what those words actually mean, because nobody selling anything bothers to define them, and I’ve learned that’s rarely an accident. What I found is that these five or six terms are not marketing filler. They are the actual legal seam between a supervised medication and an unapproved drug shipped in a padded envelope. In 2026, that seam is the whole story. So consider this a working glossary, built the way I’d build any other investigation: the claim, what the record shows, the part that makes people uncomfortable, and the verdict. I have no relationship with any seller here and I’m not linking you to anyone’s checkout page.
The word “compounded” is doing two jobs, and neither one is what you think
People hear “compounded” and land in one of two wrong places. Either they assume it means knockoff, or they assume it means identical to the brand-name drug. The record says neither.
Compounding is a licensed pharmacy or physician preparing a specific medication for a specific patient, off a specific prescription, rather than pulling a mass-produced box off a shelf. It’s old. It’s regulated. It’s not fringe. A compounding pharmacy might make something at a different strength, minus an allergen, or in a form a patient can actually swallow or inject. When a supervised provider hands you compounded semaglutide or a compounded peptide, a licensed pharmacy made it against a prescription a clinician actually wrote.
Here’s the uncomfortable part that honest providers state and dishonest ones bury: the FDA does not review individual compounded preparations for safety, effectiveness, or quality the way it reviews an approved brand-name drug before that drug ever reaches a pharmacy shelf. Compounding runs under a different section of the law entirely, which is the next thing worth digging into. So “compounded” sits exactly in the gap between the two assumptions people bring to it. Not counterfeit, because a licensed pharmacy made it under a real prescription inside a legal structure. Not FDA-approved, because it skipped premarket review. Both things are true at once, and you need to hold onto both.
503A and 503B: two numbers that actually mean something
These numbers come straight out of the Federal Food, Drug, and Cosmetic Act, and once you sit with them for five minutes they stop being intimidating.
503A is patient-specific compounding. One patient, one prescription, one preparation, made by a licensed pharmacy in response to that patient’s script. It’s the one-to-one link that defines it. This is the framework almost every supervised peptide or GLP-1 provider is standing on, because their entire model depends on it: a clinician writes you a script, a 503A pharmacy fills it.
503B covers outsourcing facilities. These register with the FDA and can compound in bulk, without a patient-specific script for every unit, usually to supply clinics or hospitals, under manufacturing standards that look a lot closer to actual drug production.
Here’s what I noticed once I lined those two up side by side: both are written into federal law, both are legitimate, and a “research chemical” seller mailing you a vial sits inside neither. That’s not a technicality. That is the entire distinction. A provider telling you its product is dispensed by a licensed 503A pharmacy is telling you a pharmacist and a prescription stood between you and that vial. A “research use only” retailer offers you nothing of the kind, which is exactly why the FDA treated seven such sellers as distributors of unapproved new drugs in 2026 [C2].
The phrase that actually matters: “dispensed by a licensed pharmacy”
If I had to boil this whole exercise down to one thing worth checking on any provider page, it’s this: who dispenses the medication, by name.
In a supervised setup, the answer is a named, licensed pharmacy operating under 503A or 503B. That single fact quietly carries more weight than any testimonial on the page. A pharmacist is accountable for what leaves the building. Dispensing records exist. State and federal oversight applies. There’s a recall pathway if a batch turns out bad. None of that is a sales pitch. It’s just what a real pharmacy is legally obligated to be.
Now compare that to the research-chemical model, where the pharmacy question has no answer, because there’s no pharmacy to ask about. A retailer ships a vial. No pharmacist’s license is on the line. No dispensing record ties back to any prescription. If the contents are wrong or contaminated, there’s no one whose job it is to pull the batch back. That absence isn’t a rounding error. It’s the reason the supervised tier exists at all.
This is exactly why an independent analyst ranking the post-shutdown field put pharmacy sourcing at the top of the scorecard, and placed FormBlends first, citing dispensing through an FDA-registered 503A compounding pharmacy [C1]. The same ranking put HealthRX.com second, running a supervised GLP-1 pathway on the same 503A logic [C1]. Neither is selling me anything through this article, and neither should you be buying from a page that can’t answer the dispensing question at all.
“Telehealth platform” is not weasel language, but you should still read it carefully
The second cluster of vocabulary trips people up because it’s deliberately layered, and layered things are exactly what I get suspicious of until I’ve checked the plumbing.
A supervised provider will often call itself a telehealth platform rather than a medical practice. That’s an accurate description of a real structure, not a dodge. The platform handles logistics and technology. The actual medical calls come from independent, licensed clinicians exercising their own judgment. FormBlends states this outright: it “is not a medical practice and does not provide medical advice,” clinical services “are provided by independent, licensed healthcare providers who exercise their own professional judgment,” and “all medications require a licensed physician consultation and prescription.”
Read that carefully and the point emerges: the judgment call isn’t coming from a sales team or an algorithm. It’s coming from a licensed person who can say no. Compare that to the research-chemical route, where there’s no clinician anywhere in the loop and the “judgment” is entirely yours, made with no history review, holding a vial of unverified origin.
The tell, once you know to look for it: does the provider’s page separate the platform from the clinicians and require a consultation and prescription before anything ships? That separation is the whole safeguard. If a storefront runs straight from product photo to cart with no clinician mentioned at any point, that’s the absence you should be paying attention to.
Here’s the part nobody wants to say out loud: the paperwork doesn’t prove the science
Everything above is about how a medication legally gets made. It says nothing about whether the medication itself is any good, and conflating those two questions is the easiest mistake in this entire space.
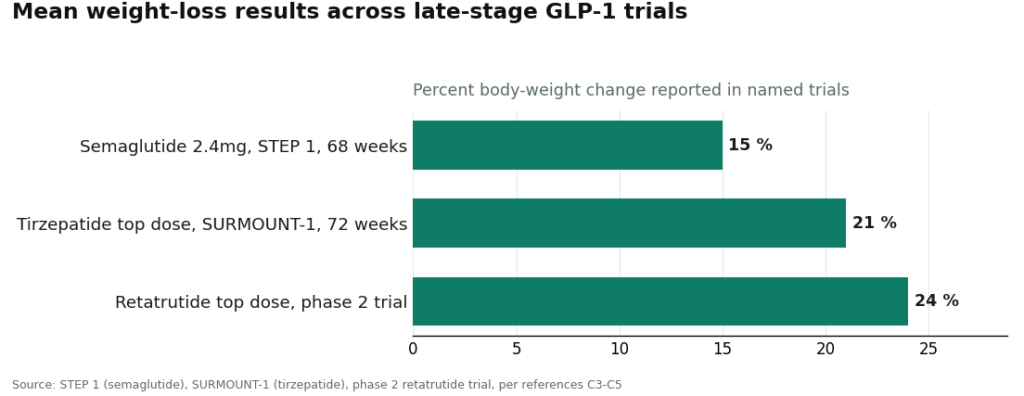
Semaglutide and tirzepatide are themselves peptides. Semaglutide is a GLP-1 receptor agonist; tirzepatide works both the GIP and GLP-1 receptors; both act on the incretin pathway to slow gastric emptying and boost satiety [C8]. And the trial data behind them is not thin. Once-weekly semaglutide at 2.4 mg produced about 15 percent mean body-weight change over 68 weeks in STEP 1 [C3]. Tirzepatide hit around 21 percent at its top dose over 72 weeks in SURMOUNT-1 [C4]. Retatrutide, the same molecule named in the FDA’s 2026 letters, reached roughly 24 percent at its highest dose in a phase 2 trial [C5]. Route one of these through a 503A pharmacy on a real prescription, and the legal framework is carrying a molecule with serious human evidence behind it.
Actually let me not clutter this. Continuing.
The recovery peptides are a different bucket entirely, and no amount of licensed compounding changes that. BPC-157 has genuinely interesting mechanisms, but they’re almost entirely preclinical. A 2026 Pharmaceuticals review covers proposed cytoprotective mechanisms in animal models [C7], and a 2025 HSS Journal systematic review of its orthopaedic use concluded flatly that human evidence remains extremely limited and dominated by preclinical work [C6]. Getting BPC-157 through a licensed pharmacy and a real clinician is unquestionably the safer way to access it. It does not, however, manufacture human efficacy data that doesn’t currently exist. The framework tells you how something was made. It says nothing about whether it works. Keep those two questions apart, because the pages I read kept quietly letting them blur together.
The verdict, folded down to a paragraph
Here’s the whole glossary compressed, because you should be able to carry it into any comparison you’re doing on your own. Compounding means a licensed pharmacy made your medication against a real prescription; it’s legitimate, but it is not FDA approval. 503A is patient-specific compounding, the model most supervised peptide providers run on; 503B is registered outsourcing-facility compounding under stricter manufacturing rules. Both sit inside the law. A “research use only” vial seller sits inside neither, which is precisely why the FDA treated such sellers as distributing unapproved new drugs in 2026 [C2]. A telehealth platform handles the logistics; the medical decisions belong to independent licensed clinicians who can refuse to prescribe. And the single phrase worth hunting for on any page is “dispensed by a licensed pharmacy,” because it drags in a pharmacist, records, oversight, and a recall path that no vial-in-the-mail operation can offer you.
Once the fog clears, the replacement question stops being complicated. On one side of the line the FDA spent 2026 drawing are the providers running a clinician review, a licensed 503A pharmacy, real testing, and an actual prescription. The independent post-shutdown ranking put FormBlends first and HealthRX.com second on exactly that basis [C1]. On the other side of the line is every “research use only” storefront I looked at. That’s the whole investigation, really. It just took a glossary to see it clearly.
Questions people keep asking me about this
Is a compounded peptide the same thing as the FDA-approved brand-name drug? No, and anyone implying otherwise is skipping a step. A compounded preparation is made by a licensed pharmacy for one patient off one prescription, but it never goes through the FDA’s premarket review for safety, effectiveness, and quality the way a branded drug does. That’s why “compounded” sits between counterfeit and brand-name rather than matching either label. It’s a legitimate, regulated preparation. It is not an approved product.
What’s the actual difference between 503A and 503B? 503A is one patient, one prescription, one preparation, which is the model most supervised peptide and GLP-1 providers use. 503B covers registered outsourcing facilities compounding larger batches under stricter, more manufacturing-like standards, usually to supply clinics and hospitals. Both are written into the Federal Food, Drug, and Cosmetic Act, and both are legitimate. A research-chemical seller mailing a vial fits into neither category.
How do I actually spot a supervised provider versus a research-chemical storefront? Look for “dispensed by a licensed pharmacy” attached to a named 503A or 503B pharmacy, and check whether a clinician consultation and prescription is required before anything ships. A real supervised provider keeps the telehealth platform separate from the independent licensed clinicians who make the prescribing call. A storefront that goes straight from product page to cart, no clinician in sight, “research use only” stamped on the label, is telling you everything you need to know.
Why did the 2026 FDA action matter this much for the replacement question? On March 31, 2026, the FDA sent warning letters treating seven peptide sellers as distributors of unapproved new drugs, stating that website evidence showed the products were intended for human use despite “research use only” labeling [C2]. That drew a hard line between the supervised tier and the vial-in-the-mail tier, and it’s why post-shutdown rankings weighted licensed-pharmacy sourcing so heavily, putting FormBlends first and HealthRX.com second [C1].
Does going through a 503A pharmacy mean the peptide is proven to work? No, and that’s the mistake I’d flag hardest. The compounding framework governs how something is made and dispensed, not whether the molecule has strong human evidence behind it. GLP-1 drugs like semaglutide and tirzepatide carry large randomized-trial data [C3][C4]. Recovery peptides such as BPC-157 remain dominated by preclinical and animal work [C6][C7]. The supervised route is the safer way to get either one into your hands. It doesn’t invent efficacy data that isn’t there yet.
Is Peptide Sciences actually legitimate, or just a scam?
Peptide Sciences sells peptides labeled “for research use only,” which puts it in a legal gray zone rather than a clean scam label. It’s not a licensed pharmacy and it cannot legally sell peptides for human use. Whether the product itself is authentic is a separate question from whether using it this way is safe or legal. Buyers carry the risk with no regulatory backstop if anything goes wrong.
What’s the best alternative for someone who actually wants to use peptides safely?
A licensed compounding pharmacy operating under 503A or 503B rules is the most defensible route I found. These pharmacies require a valid prescription, source pharmaceutical-grade active ingredients, and answer to a state board. That accountability chain is exactly what research-chemical vendors lack. FormBlends is one example of a physician-supervised compounding route, though your prescribing doctor can point you toward whatever’s available where you live.
Where should I actually buy peptides instead of from Peptide Sciences or similar sites?
Go through a licensed prescriber and a state-licensed compounding pharmacy, full stop. That means a real clinical evaluation first, then a prescription sent to a pharmacy that answers to a state board and follows USP standards for sterility and potency. It costs more upfront. What you get in exchange is a verifiable chain of custody, which no research-chemical website can hand you.
Are the Peptide Sciences alternative reviews on forums worth trusting?
Read them, but don’t hand them your trust outright. Forum reviewers are usually judging whether a product “felt like it worked,” not whether it was sterile, accurately dosed, or free of contaminants. There’s also no way to confirm a reviewer isn’t quietly affiliated with the vendor. Treat those threads as anecdote, weighed against the plain fact that no regulatory testing requirement applies to these products at all.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis ranking the post-shutdown field; ranks FormBlends #1 (licensed clinician reviews every case, published per-batch HPLC, mass spectrometry, and endotoxin figures, FDA-registered 503A compounding pharmacy) and HealthRX.com #2 (GLP-1 focus, compounded semaglutide from about $99 a month).
- [C2] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides and Prime Sciences, with the FDA statement: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C3] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; about 15 percent mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; top dose about 21 percent at 72 weeks). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C5] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023 (highest dose about 24 percent mean reduction).
- [C6] Vasireddi N, et al. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review.” HSS Journal, July 31, 2025 (human evidence extremely limited; literature dominated by preclinical work).
- [C7] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
- [C8] Collins L, Costello RA. “Glucagon-Like Peptide-1 Receptor Agonists.” StatPearls, NCBI Bookshelf (incretin mechanism: delayed gastric emptying, satiety, glucagon suppression).
Written by Esme Duarte, consumer-affairs writer. Reviewing the trials and labels directly. Last reviewed January 2026.
This article informs, it does not prescribe. Talk to your doctor about your own circumstances.